A biller who's spent ten years coding office visits and annual physicals will freeze the first time an anesthesia record lands on their desk. Start times, stop times, base units, and modifier stacks that determine who gets paid what percentage. None of it looks like the CMS-1500 workflow they know. That gap is a big reason anesthesia claims get denied at higher rates than almost any other specialty, and why practices treating it like ordinary billing tend to lose money quietly, month after month. The 2026 Medicare anesthesia conversion factor sits at $20.4976 per unit, according to the American Society of Anesthesiologists (2025), separate from the standard physician fee schedule conversion factor. That's not a rounding quirk.
It signals that anesthesia runs on its own payment system, and understanding anesthesia billing vs medical billing starts with accepting that the two were never built to work the same way.
Traditional medical billing, the kind used for office visits, surgeries, and most outpatient care, works off a fee schedule tied to a single CPT code per service. A physician performs a knee replacement, assigns the matching CPT code, and the payer reimburses a fixed rate for that procedure, adjusted by geography and a handful of modifiers.
Documentation supports what happened, coding translates it, and claims go out on the CMS-1500 form, or the UB-04 if a facility bills for the encounter instead of the provider. This guide to professional claims vs institutional claims breaks down who submits what.
Reimbursement here is largely static. One code, one rate, minor variation for complexity. A well-trained biller can move between specialties without much retraining, because the underlying revenue cycle logic barely changes even when the clinical content does.
Anesthesia breaks that pattern almost entirely. Instead of billing a flat rate per procedure, anesthesia providers bill for the entire span of time spent managing a patient's care, from the moment anesthesia begins until the patient is handed off in recovery. That single shift is a reason anesthesia billing services exist as a distinct specialty rather than a subset of general practice billing.
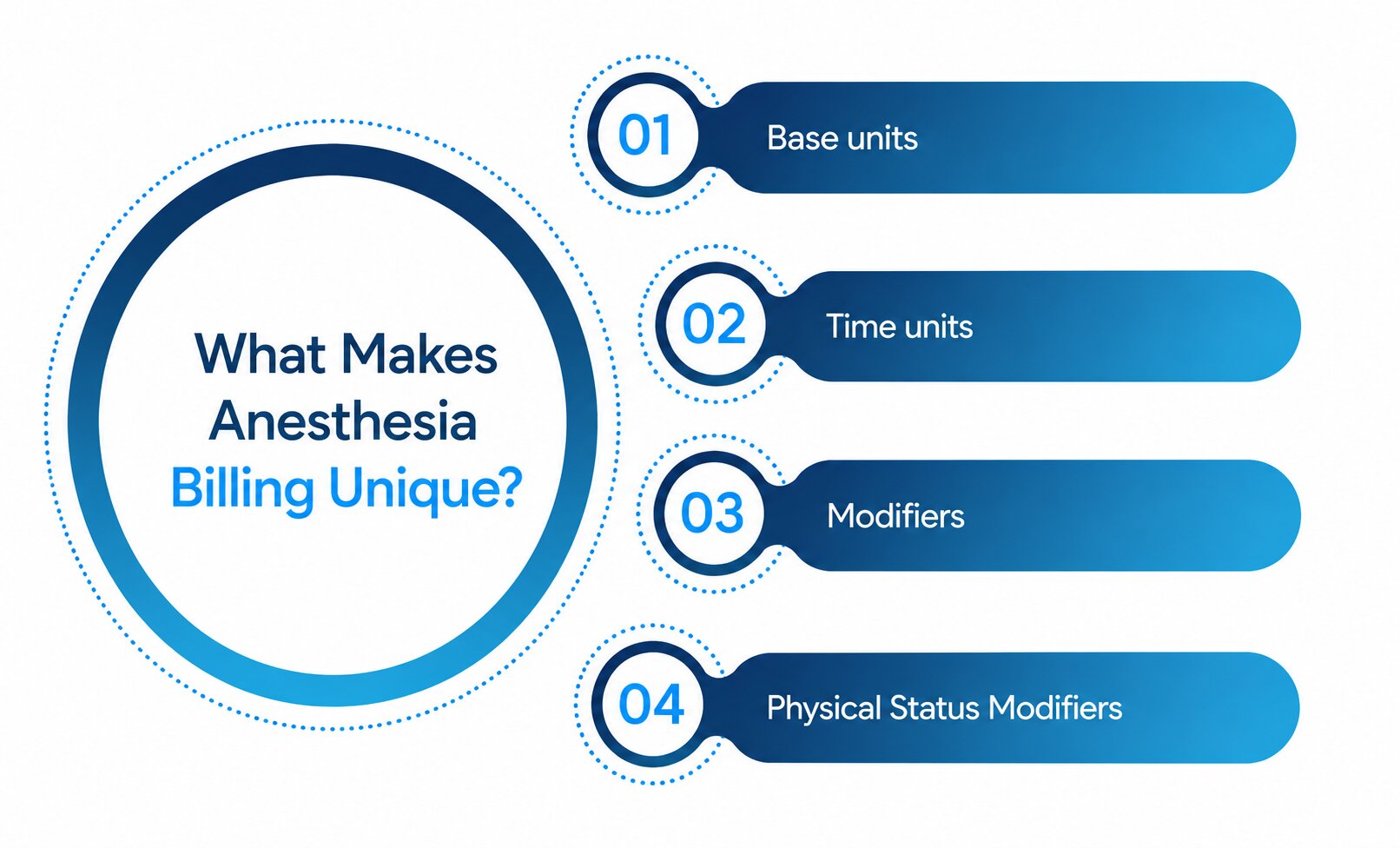
A few elements combine to build the final reimbursement, and each carries its own risk of error.
Every anesthesia CPT code, ranging from 00100 to 01999, carries a fixed value reflecting the complexity of the surgery. A simple procedure might sit at three or four units, while a complex cardiac case can climb into the high teens.
Anesthesia time is tracked in minutes and converted into units, usually in 15-minute increments, depending on the payer. A long case adds units, a short one subtracts them, so the clock has to match the anesthesia record precisely.
Codes like AA, QK, QX, and QZ tell the payer whether the anesthesiologist worked alone, medically directed a CRNA, or something in between. Get it wrong and the whole claim can shrink or get denied outright.
P1 through P6 reflect how medically complex the patient was heading into surgery. Medicare skips extra payment here, but many commercial payers don't, so identical cases can generate different revenue depending on who's paying.
Provider roles complicate things further. An anesthesiologist working solo bills differently than one medically directing several CRNAs at once, and if a fifth concurrent case starts before the fourth closes, the whole billing structure shifts to medical supervision at a lower rate. Most general billers have never had to track anything like that.
Explore a detailed 2026 guide to anesthesia billing services.
Laid side by side, the contrast is stark enough to question why anyone assumes the two can be handled by the same team without extra training.
|
Category | Traditional medical billing | Anesthesia billing |
|
Billing methodology | Flat rate per CPT code | Base units plus time units plus modifiers |
|
Time tracking | Not typically required | Precise start and stop times, minute by minute |
|
Coding | Single procedure code | Anesthesia-specific codes (00100 to 01999) tied to the surgical procedure |
|
Documentation | Procedure notes and diagnosis codes | Anesthesia record, concurrency logs, provider involvement notes |
|
Modifiers | Standard modifiers (25, 59, and similar) | Staffing modifiers (AA, QK, QX, QY, QZ) plus physical status modifiers |
|
Reimbursement | Fixed fee schedule amount | Variable, calculated per case from units and conversion factor |
That table doesn't capture everything, but it shows why treating anesthesia billing vs medical billing as a minor variation rather than its own discipline sets practices up for underpayment before a claim goes out.
Time-based reimbursement sounds simple until documentation and the OR clock disagree. Say a CRNA administers anesthesia for a laparoscopic cholecystectomy. The surgical record shows 95 minutes, but the anesthesia record, kept separately, shows 110 minutes because it includes pre-induction monitoring that the surgical team never tracks. Submit 95 minutes because that's what the operative report shows, and the claim underbills by roughly a full unit. Across a month of cases, that adds up.
This is also where things get genuinely uncertain. Time rounding rules, whether a payer uses 10-minute or 15-minute increments, and how physical status units get treated vary by payer contract. No single federal standard applies across the board, and a biller who assumes Medicare's rules apply everywhere will misbill commercial claims without realizing it.
The most persistent myth is that a biller solid on general cpt codes for anesthesia work can pick up anesthesia claims without much of a learning curve. That's rarely true. Documentation requirements, concurrency tracking, and modifier logic take real time to master, and mistakes untrained billers make aren't always obvious until an audit flags them months later.
A second misconception treats anesthesia denials the same as denials anywhere else. They rarely share the same root causes. Modifier and time-unit errors dominate here in a way that eligibility issues rarely do elsewhere, so the fix has to match how these claims are built.
Anesthesia billing was never meant to mirror the rest of medical billing, and treating it that way is how practices quietly leave revenue on the table. Differences in time tracking, modifiers, and provider roles demand a level of specialization that general billing training doesn't provide, which is why understanding anesthesia billing vs medical billing matters before a single claim goes out the door.
Practices that want to see where their own anesthesia claims might be losing units or mismatched modifiers can start with a closer look at last quarter's denial patterns through RCM Matter's anesthesia billing specialists.
1. What is the difference between anesthesia billing and medical billing?
Traditional medical billing pays a flat rate per procedure code. Anesthesia billing calculates reimbursement from base units, time units, and modifiers, a different calculation entirely, not just a different code set.
2. Why is anesthesia billing time-based?
Because anesthesia care runs continuously rather than happening as a single discrete event. A provider manages the patient throughout the case, and reimbursement reflects the actual duration of that involvement.
3. Are anesthesia claims coded differently?
Yes. Anesthesia uses its own CPT code range, 00100 through 01999, tied to the surgical procedure rather than the anesthesia service itself. That quirk trips up a lot of new billers.
4. Why are modifiers important?
Honestly, they're the single biggest point of failure in anesthesia claims. Staffing modifiers determine what percentage of the allowed amount gets paid, and using the wrong one can cut reimbursement in half or trigger a flat denial.
5. Is anesthesia billing more complex than general medical billing, and can general billers handle it?
Most experienced RCM professionals say yes to the first half and not without training to the second. Anesthesia billing involves more moving parts and payer-specific variation than general billing doesn't demand, though a biller with solid general experience can learn it with enough deliberate repetition.
Optimize billing, claims and collections with expert RCM support let our professionals handle the process so you can focus on patient care.



